
Understanding Autoimmune Arthritis: What Your Body Might Be Telling You
Many people think that arthritis is simply a condition that comes with age. You’ve walked too much, your knees are creaky, your hands are swollen a bit in the morning; you chalk it up to your years on this earth. And sometimes, that’s all it is. But then, there’s another kind of arthritis that has nothing to do with wear and tear and can appear at any age.
Autoimmune arthritis is when the immune system – that’s supposed to keep you healthy by fighting foreign invaders – misfires into attacking the very tissues it’s supposed to protect. It sounds weird because it is weird. Your body considers your joint tissue the enemy and wages war against it.
The only catch? The symptoms aren’t too different from ordinary arthritis, to begin with. No wonder so many people go months (years!) without a diagnosis.
This is the Difference that Actually Matters
Osteoarthritis develops from wear and tear of the joints over time. You’ve used your knees for decades; cartilage breaks down; bone-on-bone is the result. It’s mechanical.
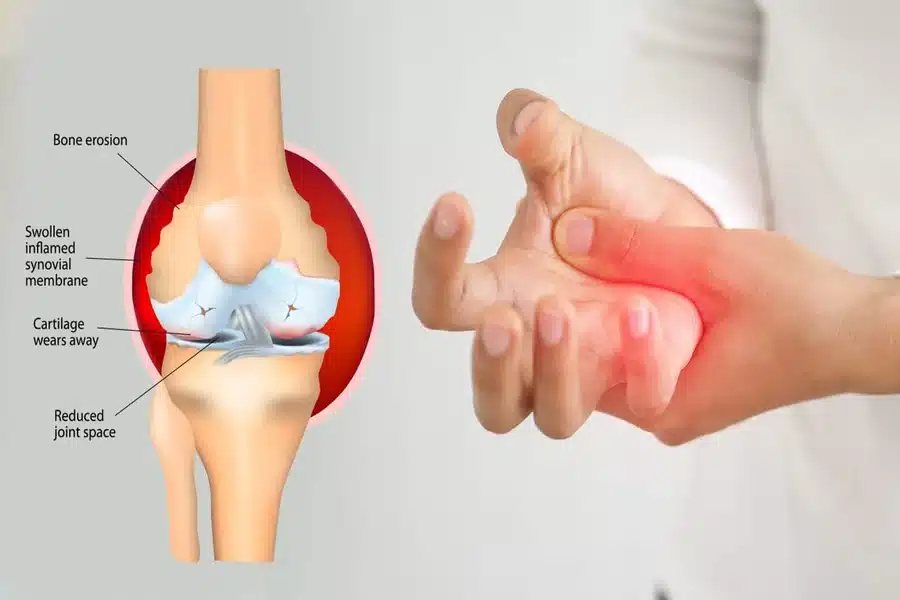
Autoimmune arthritis – includes rheumatoid arthritis, psoriatic arthritis, and a few others – are entirely different beasts. They are inflammatory. The immune system mounts antibodies and inflammatory proteins that attack the joint lining; this causes inflamed, painful joints and can alter joint structure, as well.
That’s why this distinction means so much: autoimmune arthritis is progressive. Without treatment, it continues to ruin joints. With effective treatment, you can slow down or halt that progression. As for osteoarthritis? There’s no prevention – only symptom management and hoping to keep what you have.
Autoimmune arthritis can change course with proper medication.
What Your Body Might be Trying to Say
So, what are the most common symptoms of autoimmune arthritis? They’re sneaky, starting slow enough for people to not realize something is awry until they are in too deep.
For example, morning stiffness is a classic red flag. We’re not talking about stiffness for five minutes until you get up and around; we’re talking an hour or more of stiffness too painful to move your hands or knees effectively. Some patients report their hands feeling like they’re in gloves that are three sizes too small.
Pain also feels different. It’s not a dull ache from overuse; it hurts deep within and doesn’t subside with rest. And this is where people are taken aback: the joints feel warm and are swollen red or puffy as well.
Symmetry applies. If both wrists hurt; or both sets of knuckles hurt; or both knees – these are more common with autoimmune arthritis; normal wear-and-tear generally shows up on one side first or with overworked joints.
But it’s not just about the joints, either. Many people note they’re exhausted when they wake up – but sleep doesn’t do them better. They’ll run a slight fever without being sick; get rashes or dry eyes. It would make sense; autoimmune conditions mean systemically your body’s inflamed.
When Things Don’t Seem Right
There’s a weird gap that exists between knowing something is wrong, but nothing helps and being treated by professionals for imaging or medication that also comes back normal at first.
Someone might try over-the-counter pain medications; minimize movement of the impacted joint, and ice it. They go to their primary care physician who also orders x-rays. In autoimmune arthritis, images are usually normal – in this stage – and there’s no damage yet assessed, although the inflammatory process is well underway. This is where treatment can be stalled for months when one person’s joints silently have ulterior motives.
Reaching a rheumatologist sooner in this process can change everything since they know what blood tests to run (and specific antibodies and inflammatory markers they’re looking for) and can connect symptoms that seemingly don’t connect. They also know that treatment works best before definitive joint damage occurs.
The Blood Work & Imaging Required
Blood work isn’t just one test; it’s a myriad of tests in conjunction with clinical assessment over time. The first things doctors look for are inflammatory markers like C-reactive protein and erythrocyte sedimentation rate (the latter is how they measure inflammation). They also look for rheumatoid factor or anti-CCP antibodies, which show presence in many patients with rheumatoid arthritis.
But here’s the caveat: not everyone has positive antibody tests early on – or at all! Some people are “seronegative” meaning their blood looks fine, but their presentation screams otherwise.
That’s why clinical information matters! A knowledgeable professional knows what they’re doing when they assess the pattern of symptoms and get the ball rolling for treatment even if lab work says otherwise for the time being.
Imaging has improved. Plain x-rays show little progression at first, but ultrasound and MRI can see joint lining inflammation before permanent damage occurs – which helps prevent damage sooner rather than later.
What Treatment Looks Like
Things have drastically changed in recent decades for autoimmune arthritis treatment since it was less about medications and more about pain management before essentially hoping for the best. Nowadays, there are pharmaceutical options that can modify the course of the disease.
Most start on disease-modifying drugs that calm down inflammation attacking the joints. These aren’t as much pain medications as they are aimed at stopping the underlying inflammatory process. They can be pills or injections/infusions that take a few weeks or months for significant effects – which is frustrating when you’re currently in pain.
In the meantime, anti-inflammatory medications or short courses of steroids might regulate symptoms while the longer-acting medicines kick in since treatment should get inflammation under control as soon as possible.
Newer biologic medications have been game-changers for many. These target specific immune responses driving joint inflammation – helping many who didn’t respond to older treatments in unique ways.
But medication is only part of it; physical therapy maintains joint flexibility and strength while occupational therapy seeks better means of doing day-to-day acts with less tension on impacted areas. Diet and exercise matter – a stable weight reduces pressure on joints but activity (done properly) ultimately helps inflammation.
Living With Autoimmune Arthritis
Most don’t tell patients this enough up-front: it’s manageable but chronic. There’s no cure; there’s ongoing treatment and observation.
That sounds intense – but many find their new normal with relative ease. Eventually, you learn what’s best and adapt to symptoms when they’re bad while taking proactive approaches to combat them before they start. Many get to where their disease is controlled, and they can do most things they want.
But people who see symptoms and ignore or try to experience duration later on end up with residual damage that can’t be improved. But people who get appropriate treatment early on? They do well!
The Bottom Line
If you’ve got joint pain that won’t quit; morning stiffness that lasts longer than an hour; swelling that seems relatively transient between joints – don’t chalk it up to normal aging particularly if you feel unusually fatigued or inoperable during the day.
Autoimmune arthritis is one condition where time truly matters – getting appropriate treatment early means better outcomes down-the-line as your joints will appreciate you paying attention to what they’re saying instead of waiting until fixed becomes harder than manageable.
No one wants to think they could have a chronic condition – but when you’re aware what’s actually going on – and what concrete treatment options there are instead of merely existing – day-to-day feels significantly better along with your long-term joint integrity.